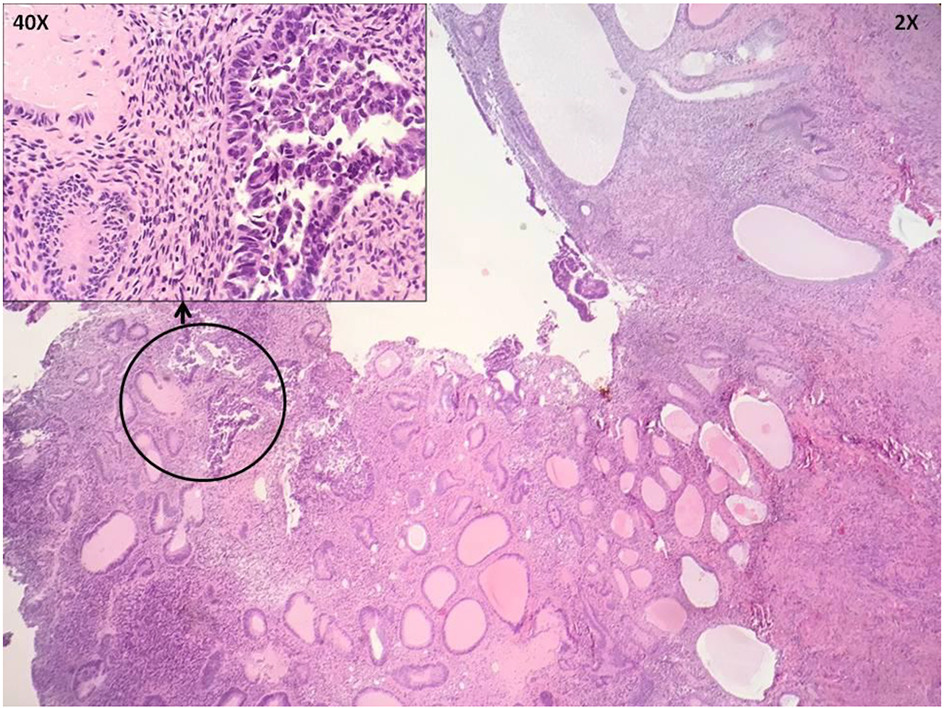
Figure 1. Hysterectomy specimen shows endometrial intraepithelial carcinoma (EIC) in an endometrial polyp.
| Journal of Clinical Gynecology and Obstetrics, ISSN 1927-1271 print, 1927-128X online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Clin Gynecol Obstet and Elmer Press Inc |
| Journal website http://www.jcgo.org |
Case Report
Volume 6, Number 3-4, October 2017, pages 71-74
Distant Cutaneous Manifestations of a Primary Gynecologic Malignancy
Figures

Table
| Months after presentation | Clinical events |
|---|---|
| EMB: endometrial biopsy; EIC: endometrial intraepithelial carcinoma; RA-TLH and RSO: robotic-assisted total laparoscopic hysterectomy and right salpingo-oophorectomy; SAR: subacute rehabilitation. | |
| 0 | Presented with vaginal bleeding, diagnosis of atypical hyperplasia on EMB |
| 1 | Underwent RA-TLH and RSO, final pathology consistent with EIC |
| 33 | Axillary lymph node recurrence on surveillance, systemic chemotherapy initiated (carboplatin and paclitaxel, followed by carboplatin and docetaxel), no evidence of disease after completion of chemotherapy |
| 40 | Recurrence of disease, single-agent chemotherapy initiated (docetaxel) |
| 47 | No response to treatment, chemotherapeutic agent changed (temsirolimus) |
| 48 | Hospital admission for abdominal pain and fatigue, cutaneous lesions noted |
| 49 | Hospital admission for bowel obstruction, exploratory laparotomy with loop colostomy, discharge to SAR |
| 51 | Death |