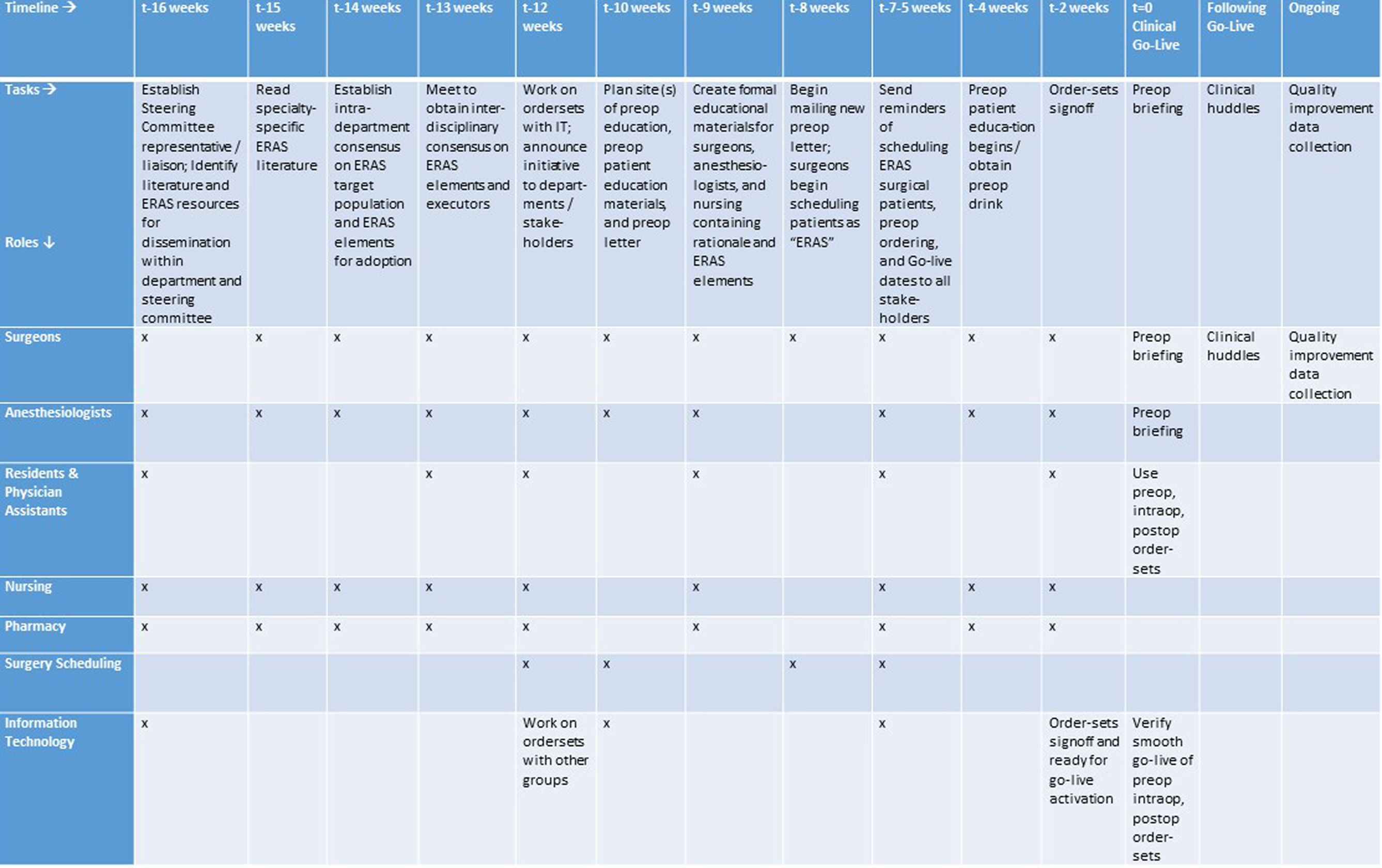
Figure 1. Implementation timeline for an enhanced recovery pathway in gynecologic surgery. In this implementation timeline, tasks are listed on the horizontal axis in chronologic order, and roles are listed on the vertical axis. The roles are fulfilled by members of the ERP steering committee and stakeholders to whom tasks apply. An ERP steering committee would typically meet every 1 - 4 weeks as full group or subgroup, and consists of the hospital-wide project manager, department project manager, and a representative for each division listed in the task role. A modification of this figure has previously been published. ERP: enhanced recovery pathway.