

| Journal of Clinical Gynecology and Obstetrics, ISSN 1927-1271 print, 1927-128X online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Clin Gynecol Obstet and Elmer Press Inc |
| Journal website http://www.jcgo.org |
Case Report
Volume 2, Number 2, September 2013, pages 93-95
Bowel Herniation Through Broad Ligament Mimicking Ovarian Torsion: A Novel Presentation
Gupta Natashaa, b, Boler Leoa, Blankstein Josefa
aDepartment of Obstetrics and Gynecology, Mount Sinai Hospital, 1500 S California Ave, Chicago, IL, 60608, USA
bCorresponding author: Natasha Gupta, Mount Sinai Hospital, Department of Obstetrics and Gynecology, 1500 S California Ave, Chicago, IL, 60608, USA
Manuscript accepted for publication June 19, 2013
Short title: Bowel Herniation Through Ovarian Torsion
doi: https://doi.org/10.4021/jcgo163w
| Abstract | ▴Top |
Ovarian torsion is an important differential diagnosis in female patients with severe, lower abdominal pain. We report a patient in whom torsion was considered. However, laparoscopy demonstrated an obstructed bowel loop adjacent to adnexa. Patient had bilateral defects in broad ligament, causing migration and incarceration of bowel on left side.
Keywords: Internal herniation; Broad ligament; Ovarian torsion; Bowel herniation; Laproscopy
| Introduction | ▴Top |
Ovarian torsion is a very common cause of unilateral, severe pain abdomen in a female patient. We report a patient who presented with such one sided severe, lower abdominal pain. Transvaginal scan is an important diagnostic tool where demonstration of a large complex, cystic mass adjacent to the adnexa will further confirm this suspicion, thus demanding an urgent surgical management. Surgery demonstrated bilateral broad ligament defects with intestinal herniation and obstruction on left side, in this patient.
Intestinal herniation through broad ligament is a very rare cause of bowel obstruction. This type of internal herniation of bowel is caused by migration of bowel through a defect in the broad ligament, either from congenital or acquired etiology. Patients usually present with signs and symptoms of bowel obstruction. A preoperative diagnosis of bowel obstruction would be very difficult in this patient, due to absence of any bowel related signs or symptomatology. This is a most unusual presentation of internal bowel herniation where its strategic location adjacent to the adnexa mimicked an ovarian torsion.
| Case Report | ▴Top |
A 27 years old Gravida2 Para2 patient, presented with sudden onset of severe left lower quadrant pain. She had no other symptoms including emesis or altered bowel habits. She had history of 2 cesarean sections and stab wounds to thorax, requiring thoracotomy in past. Patient had localized tenderness and guarding in the left lower quadrant. Pelvic examination elicited left adnexal fullness and discomfort. Her labs were normal and transvaginal scan showed a 6.07 × 4.9 × 4.09 cm left adnexal complex cystic mass with papillary projection and thick septation (Fig. 1). Color flow within septa was noted partially. A diagnosis of ovarian torsion was made based on these sonographic findings and patient’s clinical examination.
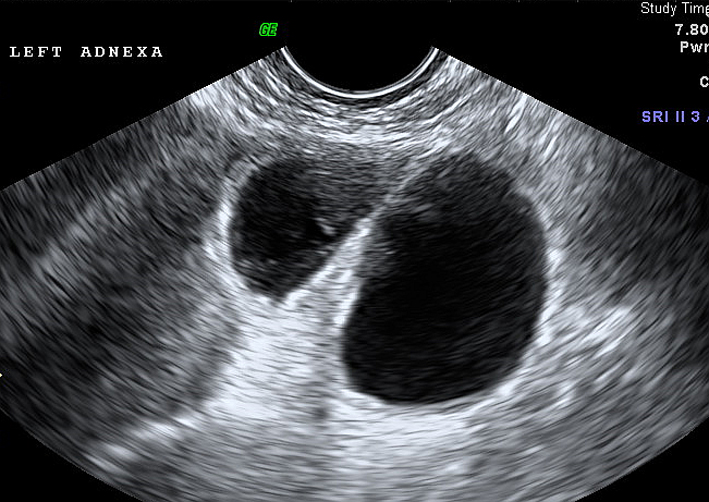 Click for large image | Figure 1. Tranvaginal scan at presentation. Transvaginal scan showing a large complex, cystic mass in left adexa, with septation. (A reconsideration of this scan in retrospect, suggests dilated incoming and outgoing loop of bowel.) |
Patient underwent a diagnostic laparoscopy, where both ovaries appeared normal. A large, bluish, incarcerated loop of sigmoid colon was noted adjacent to uterus on the left side. On manipulation of the bowel, we noticed a large, well circumscribed defect in the left broad ligament, through which bowel loop had herniated and became incarcerated (Fig. 2). A similar size, circular defect was noted in the right broad ligament, but without any herniation through it. These defects were placed, inferior to the round ligament on either side, but above uterine vessels and were bordered by broad ligament medially and laterally (Fig. 3) [1].
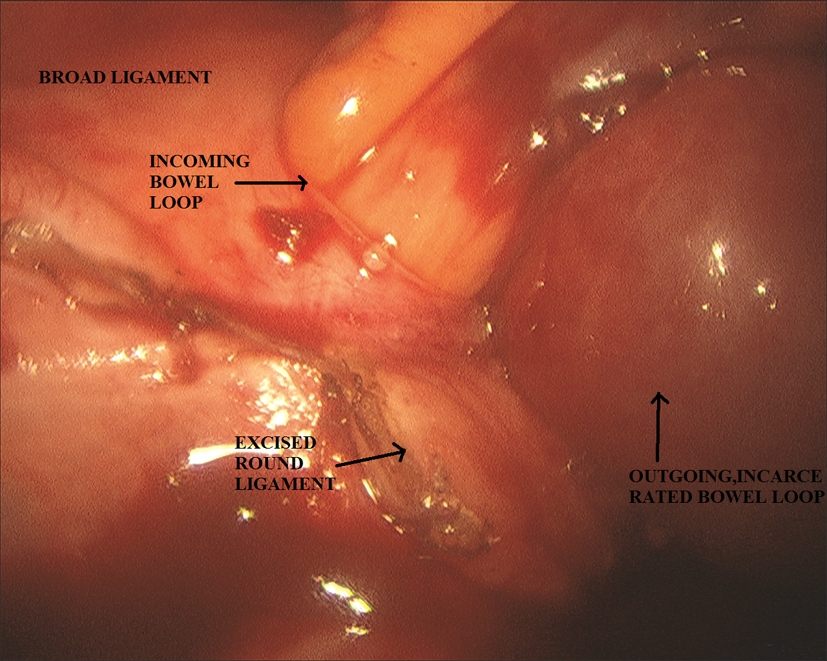 Click for large image | Figure 2. Laparoscopic findings. Intraoperative view of the herniatied bowel loop through the defect in broad ligament. |
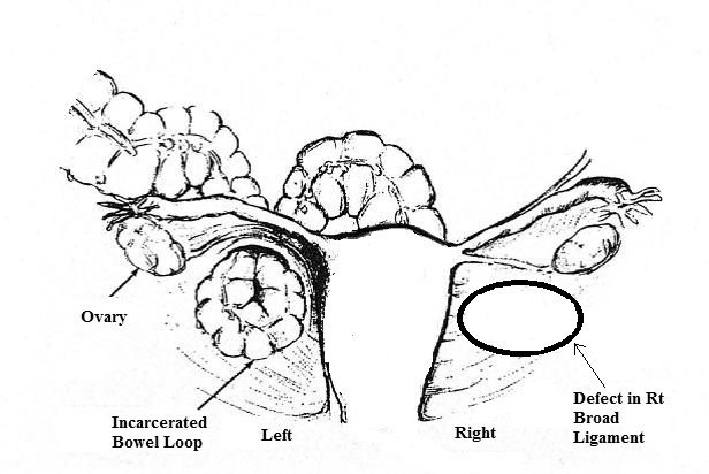 Click for large image | Figure 3. Broad ligament defects. Illustration of bilateral defects in broad ligament with bowel herniation on left side. (Modified from rabushka’s report of colon hernia through a hiatus in the broad ligament.) |
We divided round ligament on the affected side, and bowel loop was pulled out. It appeared pink and viable within a few minutes, thus avoiding resection. We opened the defects on each side by dividing the round ligament, in order to prevent future episodes of bowel migration through these defects.
| Discussion | ▴Top |
Internal herniation of bowel is a rare condition, causing approximately 1% of all intestinal obstructions [2]. These occur most commonly through mesenteric defects. Internal herniation through a defect in broad ligament is the rarest of all internal hernias. Quain first described a case of incarcerated hernia through a breech in broad ligament in 1861, found at autopsy [3, 4]. Since then, there have been many scattered reports of internal herniation of bowel, more commonly of ileum through the right broad ligament. Majority of these patients presented with small bowel obstruction and underwent surgery whereby bowel was either resected or reduced and defect primarily repaired [5].
These defects of broad ligament may be congenital or caused by previous surgery, pelvic inflammatory disease or trauma during delivery [1, 2, 6]. They have been classified as Fenestra type (involving both leaves of broad ligament) or Pouch type (in either anterior or posterior leaf) [3]. Our patient had Fenestra type defect.
A preoperative diagnosis of this condition is extremely difficult due to its rarity. Some authors have used multi-detector CT and were able to successfully diagnose it preoperatively [7]. This is possible in patients that presented with signs and symptoms of bowel obstruction, thus necessitating a CT scan. Our patient underwent transvaginal scan due to preoperative suspicion of ovarian torsion. Furthermore, despite several reported cases of this condition in literature, there is no mention of this condition in standard books of Gynecology and Surgery.
Internal herniation of bowel through broad ligament should be considered as part of differential diagnosis in patients with suspected ovarian torsion.
Conflict of Interest
None declared.
Financial Support
None declared.
| References | ▴Top |
- Rabushka SE. Colon hernia through a hiatus in the broad ligament.Report of a case and review of the literature. Obstet Gynecol. 1968;31(2):261-265.
doi pubmed - Kanbur AS, Ahmed K, Bux B, Hande T. Jejunal obstruction and perforation resulting from herniation through broad ligament. J Postgrad Med. 2000;46(3):189-190.
pubmed - Hiraiwa K, Morozumi K, Miyazaki H, Sotome K, Furukawa A, Nakamaru M. Strangulated hernia through a defect of the broad ligament and mobile cecum: a case report. World J Gastroenterol. 2006;12(9):1479-1480.
pubmed - Leone V, Misuri D, Faggi U, Giovane A, Fazio C, Cardini S. Laparoscopic treatment of incarcerated hernia through right broad ligament in patients with bilateral parametrium defects. G Chir. 2009;30(4):141-143.
pubmed - Baron A. Defect in the broad ligament and its association with intestinal strangulation. Br J Surg. 1948;36(141):91-94.
doi pubmed - Bordenca MJ. Hernia through the broad ligament complicating pregnancy. Obstet Gynecol. 1959;13(3):311-313.
pubmed - Kosaka N, Uematsu H, Kimura H, Yamamori S, Hirano K, Itoh H. Utility of multi-detector CT for pre-operative diagnosis of internal hernia through a defect in the broad ligament (2007: 1b). EurRadiol. 2007;17(4):1130-1133.
doi pubmed
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Clinical Gynecology and Obstetrics is published by Elmer Press Inc.