aDepartment of Obstetrics and Gynecology, Kaizuka City Hospital, Osaka, Japan bDepartment of Obstetrics and Gynecology, Osaka Police Hospital, Osaka, Japan cCorresponding Author: Serika Kanao, Department of Obstetrics and Gynecology, Kaizuka City Hospital, 3-10-20 Hori Kaizuka, Osaka 597-0015, Japan
Manuscript submitted February 7, 2017, accepted February 15, 2017 Short title: IANAC for Cervical Cancer doi: https://doi.org/10.14740/jcgo435w
Standard treatment for early-stage cervical cancer (Ib2-IIa and IIb with parametrial invasion) is concurrent chemoradiotherapy and/or radical hysterectomy. The efficacy of intra-arterial delivery of neoadjuvant chemotherapy (IANAC) for this cancer remains unclear. We present three cases treated by IANAC for Ib-II stage cervical cancer, with results suggesting that IANAC is an effective treatment.
For the treatment of early-stage FIGO Ib2-IIa cervical cancer, radical hysterectomy is often chosen. However, a bulky tumor or vaginal invasion can make the surgery challenging. For cervical cancer with parametrial invasion (stage IIb), concurrent chemoradiotherapy (CCRT) with platinum-based chemotherapy is usually considered to be the standard of treatment [1].
Several studies have reported on the utility of neoadjuvant chemotherapy (NAC) for cervical cancer. NAC is reported to improve the probability of complete surgical resection, and can also inhibit micrometastases to the lymphovascular space [2], contributing to improved prognosis. However, NAC is usually performed intravenously, and NAC’s efficacy by this route is somewhat controversial.
The efficacy and safety of an alternative delivery route, by intra-arterial NAC (IANAC), is as yet unclear, largely due to a sparsity of needed studies and reports. In the limited literature that is available, IANAC is purported to be superior to intravenous NAC on the grounds that IANAC increases exposure of the tumor to higher concentrations of the chemotherapeutic agent and that IANAC significantly limits the exposure of systemic tissues [3].
To provide additional evidence for the safety and efficacy of IANAC, we herein present our experience with three cases of early-stage cervical cancer treated with IANAC, followed by radical surgery. The patients were stage Ib-II, and the IANAC treatment appears to have been both effective and safe.
Objective
This report describes the efficacy of IANAC for early-stage cervical cancer.
Methods
During the period between January of 2008 and December 2013, we treated with IANAC three patients having stage Ib2-II primary cervical cancer. Stage Ib1 cases were excluded from the IANAC protocol because they had radical hysterectomies conducted directly.
For the three Ib2-II patients discussed here, it was our consensus medical opinion, because of the bulky nature of the tumors (> 4 cm in diameter) and/or the stage of the disease (stage II with parametrial invasion and/or vaginal invasion) that there would be significant difficulty in conducting a primary radical hysterectomy. Therefore, each patient received a primary neoadjuvant treatment via IANAC, followed by radical hysterectomy.
IANAC was conducted as follows. Before chemotherapy, catheters were inserted through both femoral arteries using the Seldinger technique, with the catheter tips placed into the uterine arteries. On day 1, the chemotherapy regimen involved cisplatin (70 mg/m2) and mitomycin C (15 mg/m2). The patients received two courses of IANAC, with an interval of 3 - 4 weeks. The patients were also treated with a 5-HT3 receptor antagonist and dexamethasone, beginning 4 days following the first IANAC treatment. Adverse events occurring during chemotherapy were evaluated by the Common Terminology Criteria for Adverse Events (CTCAE; version 4.0).
Finally, the interval between the second INAC treatment and the radical hysterectomy surgery was 4 - 5 weeks.
After two courses of chemotherapy, we evaluated the clinical response of the tumor with pelvic MRI. The IANAC tumor response was evaluated by MRI using guidelines from the Response Evaluation Criteria in Solid Tumors (RECIST; version 1.1) [4]. Tumor complete response (CR) was defined as having a total disappearance of detectable tumor; a 30% or more decrease in tumor size was defined as a partial response (PR); if the tumor size was not changed significantly, the response was defined as stable disease (SD). Progressive disease (PD) was defined as having a greater than 20% increase in tumor size or the appearance of any new lesion. Additionally, we pathologically evaluated the resected specimens for tumor response, which was classified as either CR, PR, or PD.
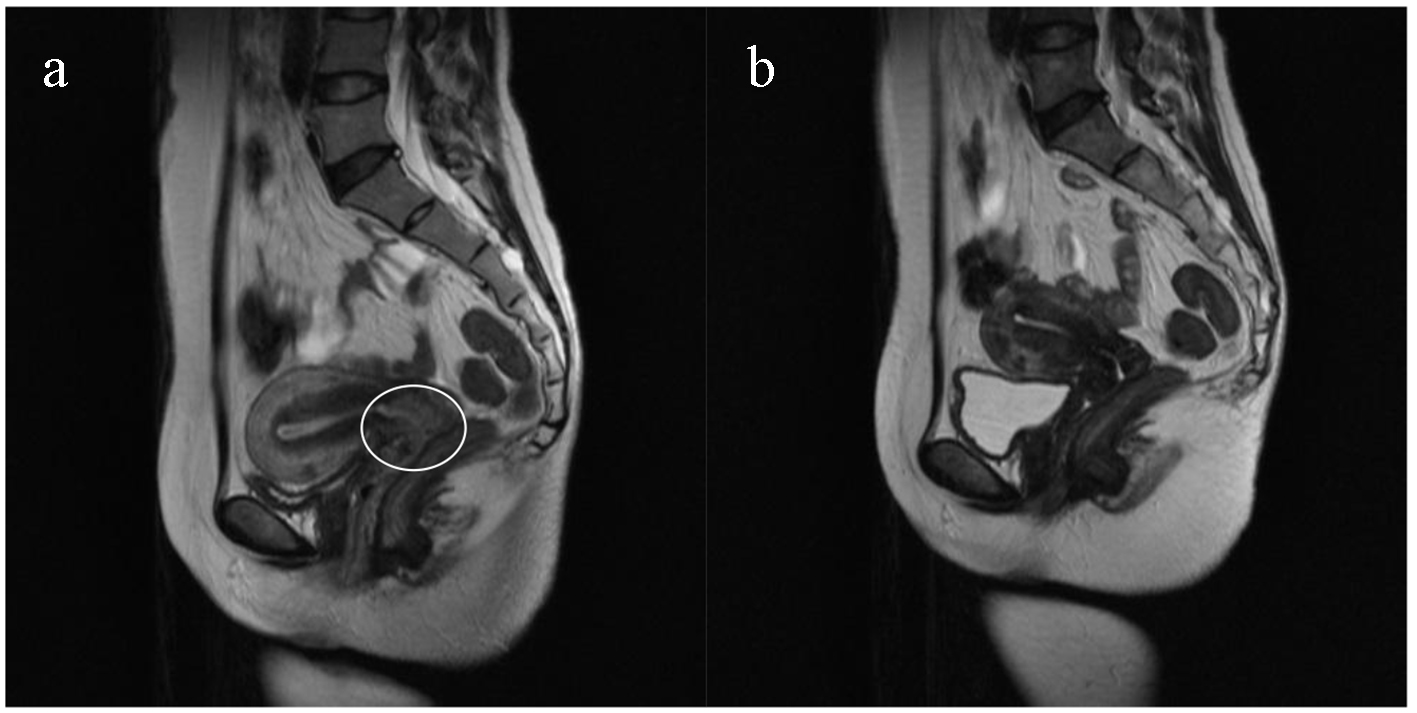
A 43-year-old woman with abnormal vaginal bleeding was referred to our hospital. Pelvic examination revealed an overt carcinoma of the uterine cervix. Colposcopy detected apparent vaginal invasion of the tumor. Biopsy indicated a squamous cell carcinoma. MRI described a 3 × 4 cm cervical tumor (Fig. 1a). Chest and abdominal CT scans found no metastatic lesions. We diagnosed this case as having FIGO stage IIa cervical cancer.
Figure 1. MRI images of case 1. (a) A T2-intensified MRI sagittal section shows the initial 3 × 4 cm cervical tumor. (b) After two courses of IANAC, the tumor has completely vanished from the same MRI section. The efficacy of NAC was judged as CR.
After two courses of IANAC, the cervical tumor had totally disappeared by MRI (Fig. 1b). We evaluated this response as CR. Adverse chemotherapy events were grade 2 nausea/vomiting on days 2 - 5. Radical hysterectomy, bilateral salpingo-oophorectomy and pelvic lymph node dissection were conducted. Pathological CR was confirmed, and no residual tumor was found in the resected specimen. No metastases to the lymph nodes and a negative vaginal surgical margin were confirmed. No adjuvant treatment was applied after the surgery. During 60 months of follow-up, there has been no sign of recurrence.
Case 2
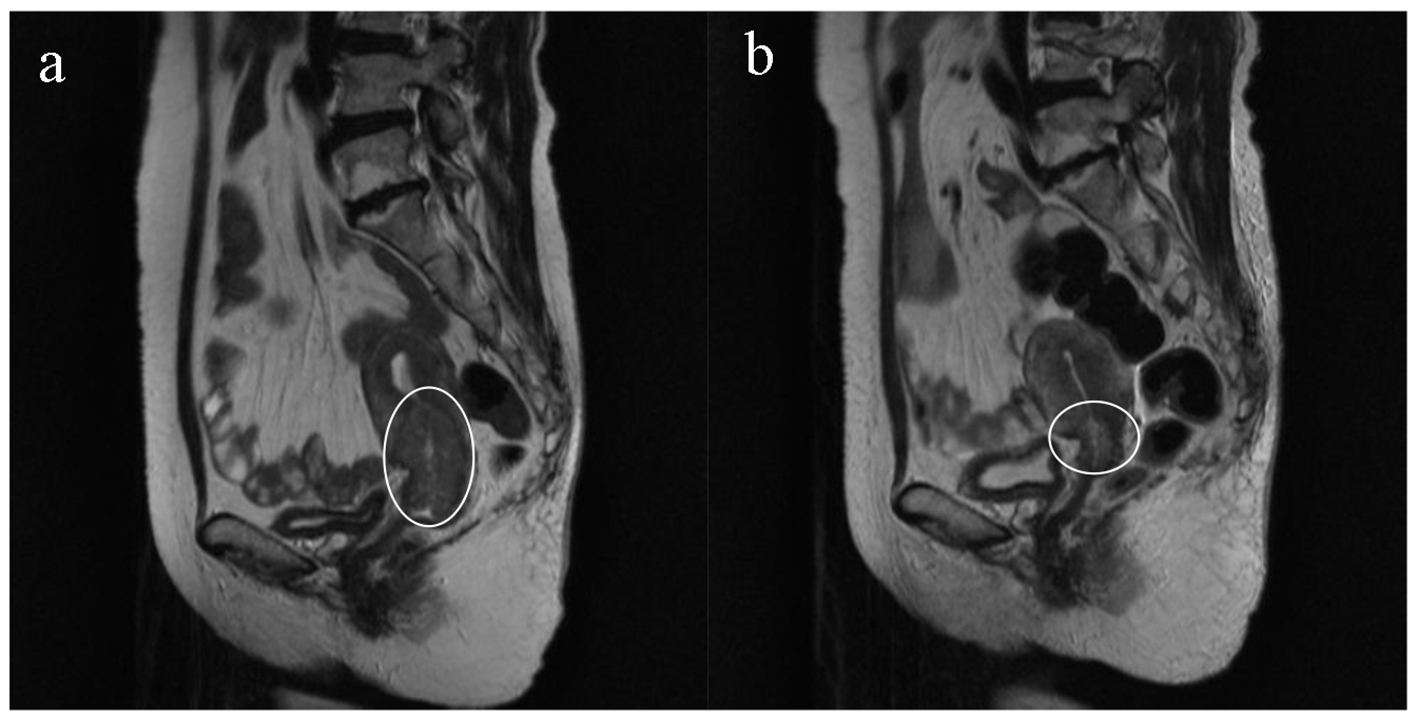
A 61-year-old woman with a symptom of recurrent vaginal bleeding visited our hospital. A cervical tumor of 5 cm in diameter was detected via internal examination and trans-vaginal ultra-sonogram. There was no parametrical invasion, as judged by digital rectal examination. Cervical biopsy indicated an adenosquamous cell carcinoma. No metastatic lesions were detected by chest and abdominal CT scans. We evaluated the case as stage Ib2 cervical cancer.
Following two courses of IANAC, MRI showed that the tumor had shrunk to 1.5 cm in diameter (Fig. 2a, b). We evaluated the response as PR. Adverse events that occurred during chemotherapy were grade 1 nausea/vomiting and grade 2 neutropenia. Following IANAC, radical hysterectomy, bilateral salpingo-oophorectomy and pelvic lymph node dissection were performed. Histopathology confirmed PR. After surgery, three cycles of adjuvant chemotherapy (cisplatin and paclitaxel) were administered. After 87 months of follow-up, no recurrence of disease has been detected.
Figure 2. MRI images of case 2. (a) A T2-intensified MRI sagittal section shows the initial 5 cm cervical tumor. (b) After two courses of IANAC, the tumor has shrunk to 1.5 cm. The efficacy of NAC was judged as PR.
Case 3
A 31-year-old woman with abnormal vaginal bleeding visited our hospital. A cervical tumor, reaching to the anterior vaginal fornix, was detected with pelvic examination. The tumor was estimated to be 3 cm in diameter by MRI. Cervical biopsy indicated a squamous cell carcinoma. No metastatic lesions were detected by chest and abdominal CT scans. We diagnosed this case as stage IIa1 cervical cancer.
After two courses of IANAC, the tumor was not detectable by MRI. The efficacy of IANAC was evaluated as CR (negative MRI images not shown). The only adverse event occurring during chemotherapy was grade 1 nausea/vomiting. After two courses of IANAC, radical hysterectomy and pelvic lymph node dissection surgery were performed. There was no tumor detected in the surgical specimen. CR was histopathologically confirmed. At 41 months post-surgery, no evidence of recurrent disease has been detected.
We present here our recent experiences with treatment of three cases of early-stage cervical cancer using the alternative IANAC delivery. We found that our patients well tolerated the IANAC treatments and subsequent radical operations, without any severe toxicity or complications, and that there has been no evidence of disease recurrence during follow-up periods ranging from 41 to 86 months. The results of these cases, although limited in number, indicate a promising efficacy of IANAC for locally advanced cervical cancer.
For cervical cancer treatments, NAC has traditionally been administered intravenously, thus systemically. There are growing numbers of reports of NAC being administered intra-arterially to directly target the downstream tumor, with the IANAC results being significantly superior to the intravenous method [2, 5]. For example, Scarabelli et al have reported IANAC response rates of 84-92% [6].
It has often been pointed out that for premenopausal women there is a possibility of toxicity to ovarian functions from administering anticancer drugs via the uterine arteries [7], although there as yet appear to be no specific reports of such IANAC-specific adverse ovarian events. Lu et al found that IANAC followed by successful laparoscopic radical trachelectomy can be a particularly useful option for women with Ib1 cervical cancer wishing to preserve their fertility [7]. All seven women they treated by IANAC in this way showed either complete or partial tumor responses.
Primary IANAC treatment provides tumor exposure to dramatically higher anti-cancer drug concentrations. For bulky cervical cancers, normally considered to be inoperable, and for cervical cancers with parametrial or vaginal invasion, more intensive neoadjuvant chemotherapy via IANAC can dramatically reduce bulk tumor volume. This makes the tumor more operable, significantly increasing the probability of a more complete tumor resection, and improves other risk factors by reducing lymph node involvement, suppressing micrometastases and recurrences, thus improving survival rates [2, 5, 8, 9].
However, some have reported otherwise, that NAC does not improve survival, and only reduces the necessity for postoperative radiation therapy [10]. This negative result may be because, although IANAC reduces drug concentration exposures to healthy systemic tissues [5], the offset disadvantage is that adequate drug concentrations may not reach potential cryptic metastatic lesions. It is unclear whether this wide discrepancy in efficacy results can be accounted for by regimental differences.
With regard to the use of IANAC for early-stage cervical cancers, studies have reported using a variety of anticancer chemotherapy regimens [11], but platinum-based regimens are still considered to be the gold standard. Kaku et al reported that CDDP (cisplatin) plus THP (cisplatin plus pirarubicin) therapy achieved a high response rate with squamous cell carcinoma, while PACF therapy (cisplatin, epirubicin, mitomycin-C and 5-flurouracil) achieved a high response rate for adenosquamous carcinoma and adenocarcinoma.
The present cases were all treated with cisplatin and mitomycin C, an INAC regimen for cervical cancer for which we can find no previous report. Based upon the apparent efficacy of this novel regimen, it should be further investigated. In particular, any adverse effects of this regimen need to be studied with larger number of cases and perhaps higher drug doses to test the upper limits of tolerability.
Reports comparing CCRT to IANAC for cervical cancer are limited. In stage IIIb cervical cancer, Kawaguchi et al showed similar survival rates between IANAC + radical hysterectomy and CCRT [12, 13]. The efficacy of IANAC makes it an attractive alternative to CCRT for treatment of locally advanced cervical cancers. In support of using this more targeted treatment approach, we have confirmed the clinical efficacy and safety of IANAC in three patients, none of whom have yet had a recurrent disease. There were no observed severe adverse events following either the IANAC or the subsequent radical surgery. Large randomized trials are needed to better evaluate the efficacy of intra-aortic NAC in the treatment of cervical cancer.
Acknowledgments
The authors would like to thank Dr. GS Buzard for his editing of this manuscript.
Conflicts of Interest
The authors declare that there are no conflicts of interest regarding the publication of this paper.
Koh WJ, Greer BE, Abu-Rustum NR, Apte SM, Campos SM, Chan J, Cho KR, et al. Cervical cancer. J Natl Compr Canc Netw. 2013;11(3):320-343. doipubmed
Wang Y, Wang G, Wei LH, Huang LH, Wang JL, Wang SJ, Li XP, et al. Neoadjuvant chemotherapy for locally advanced cervical cancer reduces surgical risks and lymph-vascular space involvement. Chin J Cancer. 2011;30(9):645-654. doipubmed
Sugiyama T, Nishida T, Hasuo Y, Fujiyoshi K, Yakushiji M. Neoadjuvant intraarterial chemotherapy followed by radical hysterectomy and/or radiotherapy for locally advanced cervical cancer. Gynecol Oncol. 1998;69(2):130-136. doipubmed
Eisenhauer EA, Therasse P, Bogaerts J, Schwartz LH, Sargent D, Ford R, Dancey J, et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer. 2009;45(2):228-247. doipubmed
Yamakawa Y, Fujimura M, Hidaka T, Hori S, Saito S. Neoadjuvant intraarterial infusion chemotherapy in patients with stage IB2-IIIB cervical cancer. Gynecol Oncol. 2000;77(2):264-270. doipubmed
Scarabelli C, Zarrelli A, Gallo A, Visentin MC. Multimodal treatment with neoadjuvant intraarterial chemotherapy and radical surgery in patients with stage IIIB-IVA cervical cancer. A preliminary study. Cancer. 1995;76(6):1019-1026. doi
Lu Q, Zhang Y, Wang S, Guo S, Guo H, Zhang Z, Liu C. Neoadjuvant intra-arterial chemotherapy followed by total laparoscopic radical trachelectomy in stage IB1 cervical cancer. Fertil Steril. 2014;101(3):812-817. doipubmed
Yamaguchi S, Nishimura R, Yaegashi N, Kiguchi K, Sugiyama T, Kita T, Kubushiro K, et al. Phase II study of neoadjuvant chemotherapy with irinotecan hydrochloride and nedaplatin followed by radical hysterectomy for bulky stage Ib2 to IIb, cervical squamous cell carcinoma: Japanese Gynecologic Oncology Group study (JGOG 1065). Oncol Rep. 2012;28(2):487-493. doi
Sevin BU, Nadji M, Lampe B, Lu Y, Hilsenbeck S, Koechli OR, Averette HE. Prognostic factors of early stage cervical cancer treated by radical hysterectomy. Cancer. 1995;76(10 Suppl):1978-1986. doi
Katsumata N, Yoshikawa H, Kobayashi H, Saito T, Kuzuya K, Nakanishi T, Yasugi T, et al. Phase III randomised controlled trial of neoadjuvant chemotherapy plus radical surgery vs radical surgery alone for stages IB2, IIA2, and IIB cervical cancer: a Japan Clinical Oncology Group trial (JCOG 0102). Br J Cancer. 2013;108(10):1957-1963. doipubmed
Kaku S, Takahashi K, Murakami Y, Wakinoue S, Nakagawa T, Shimizu Y, Kita N, et al. Neoadjuvant intraarterial chemotherapy for stage IIB-IIIB cervical cancer in Japanese women. Exp Ther Med. 2010;1(4):651-655. doipubmed
Kawaguchi R, Nakamura H, Morioka S, Ito H, Tanase Y, Haruta S, Kanayama S, et al. Comparison of neoadjuvant intraarterial chemotherapy versus concurrent chemoradiotherapy in patients with stage IIIB uterine cervical cancer. World Journal of Oncology. 2013;4(6):221-229. doi
Kawaguchi R, Tanase Y, Haruta S, Yoshida S, Furukawa N, Kobayashi H. Addition of aprepitant to standard therapy for prevention of nausea and vomiting among patients with cervical cancer undergoing concurrent chemoradiotherapy. Int J Gynaecol Obstet. 2015;131(3):312-313. doipubmed
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Clinical Gynecology and Obstetrics is published by Elmer Press Inc.