Journal of Clinical Gynecology and Obstetrics, ISSN 1927-1271 print, 1927-128X online, Open Access
Article copyright, the authors; Journal compilation copyright, J Clin Gynecol Obstet and Elmer Press Inc
Journal website http://www.jcgo.org
Case Report
Volume 6, Number 2, June 2017, pages 41-44
Hyperreactio Luteinalis in the Third Trimester Complicating Fetal Hydrops and Mirror Syndrome
Natasha Mehandrua, c, Joseph Harrisa, Olga Kalinkinb, Andrew Liguorib
aDivision of Maternal Fetal Medicine, St. Joseph’s Hospital and Medical Center, 500 West Thomas Road Suite 700, Phoenix, AZ 85013, USA bRadiology Department, St. Joseph’s Hospital and Medical Center, 350 West Thomas Road, Phoenix, AZ 85013, USA cCorresponding Author: Natasha Mehandru, St. Joseph’s Hospital and Medical Center, 500 West Thomas Road Suite 700, Phoenix, AZ 85013, USA
Manuscript submitted February 26, 2017, accepted March 16, 2017 Short title: Hyperreactio Luteinalis and Fetal Hydrops doi: https://doi.org/10.14740/jcgo439w
Hyperreactio luteinalis (HL) is a benign condition marked by bilateral ovarian cystic enlargement. It is rare and understanding its presentation will prevent unnecessary surgical intervention. A 21-year-old G1P0 with a spontaneous singleton pregnancy complicated by non-immune fetal hydrops and mirror syndrome developed abdominal pain and dyspnea. She underwent therapeutic amnioreduction at 31 3/7 weeks gestation due to presumed symptomatic polyhydramnios. An obstetric ultrasound showed large bilateral ovarian masses, maternal ascites, and a left pleural effusion. Due to abnormal fetal Dopplers, she underwent a cesarean section and ovarian biopsies at 31 4/7 weeks gestation. Pathology revealed bilateral corpus luteal cysts. New onset bilateral ovarian masses associated with HL can be seen in spontaneous pregnancies complicated by fetal hydrops and mirror syndrome, and are best treated conservatively.
Hyperreactio luteinalis (HL) is a rare complication of pregnancy. It is associated with gestational trophoblastic disease, multifetal gestation, fetal hydrops, ovarian hyperstimulation, and isoimmunization [1]. The highest incidence (10-20%) is observed in gestational trophoblastic disease [1]. HL is thought to be due to elevated β-hCG levels or an abnormal response to normal levels [1]. HL may be asymptomatic, or present with diffuse abdominal pain, nausea, emesis, pleural effusions, and ascites. The condition typically resolves following delivery [2]. HL is best managed conservatively. Differentiating the diagnosis of HL from others that mimic it, such as ovarian hyperstimulation syndrome (OHSS) and malignancy, prevents unnecessary surgical intervention.
A 21-year-old G1P0 at 28 2/7 weeks gestation by a 6-week ultrasound presented to our hospital following a new diagnosis of fetal hydrops and abnormal fetal umbilical artery Dopplers. Her past medical and gynecologic history were insignificant. Workup for fetal hydrops included rhesus positive status, negative maternal cell free DNA, and negative TORCH serology and polymerase chain reaction from amniocentesis.
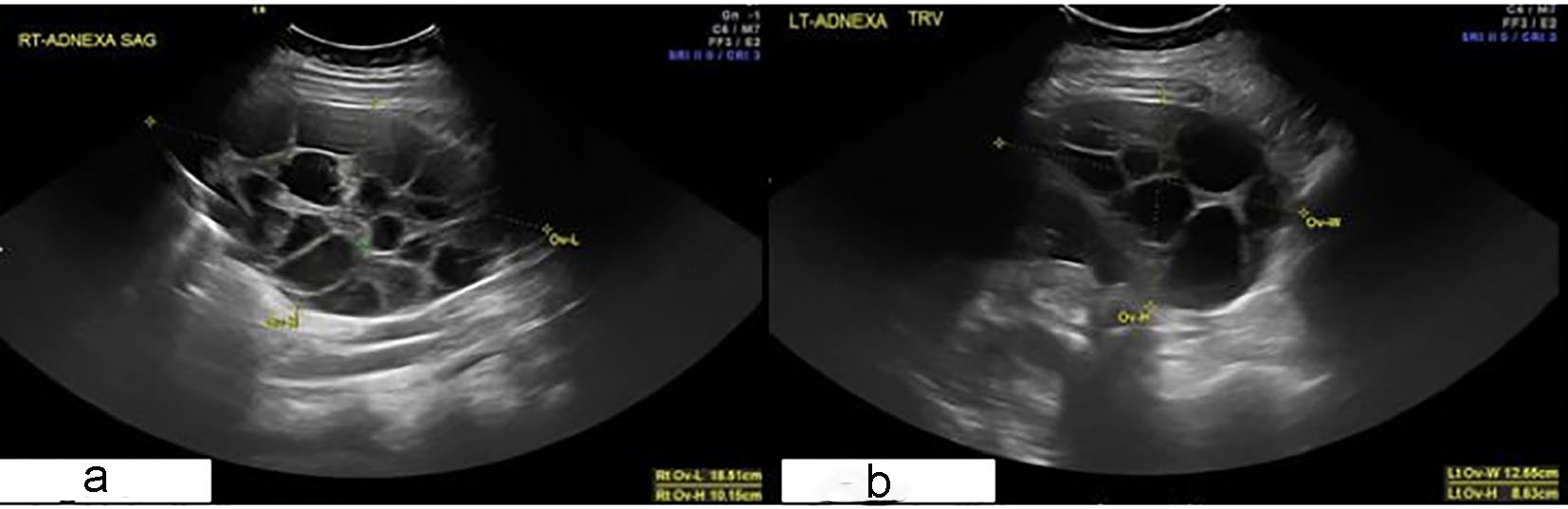
Expectant management included administration of betamethasone 12 milligrams intramuscularly every 24 hours for 2 doses to stimulate fetal lung maturity. At 30 5/7 weeks gestation, she developed nausea, vomiting, abdominal pain, and dyspnea. An obstetric ultrasound showed polyhydramnios with an amniotic fluid index of 32.5 cm. She underwent therapeutic amniocentesis twice for symptomatic relief. A follow-up obstetric ultrasound at 31 3/7 weeks gestation showed enlarged ovaries with multiple simple appearing thin walled cysts; the right ovary measured 14.4 × 12.2 × 9.2 cm and the left ovary measured 10.0 × 10.3 × 6.4 cm (Fig. 1). There was small volume maternal ascites, right lower quadrant free fluid, and a small left-sided pleural effusion.
Figure 1. Transabdominal ultrasound. Enlarged right (a) and left (b) ovaries with multiple thin walled cysts 2 days prior to cesarean section. Right ovary measures 14.4 × 12.2 × 9.2 cm; 845.2 cm3 volume. Left ovary measures 10.0 × 10.3 × 6.4 cm; 343.2 cm3 volume.
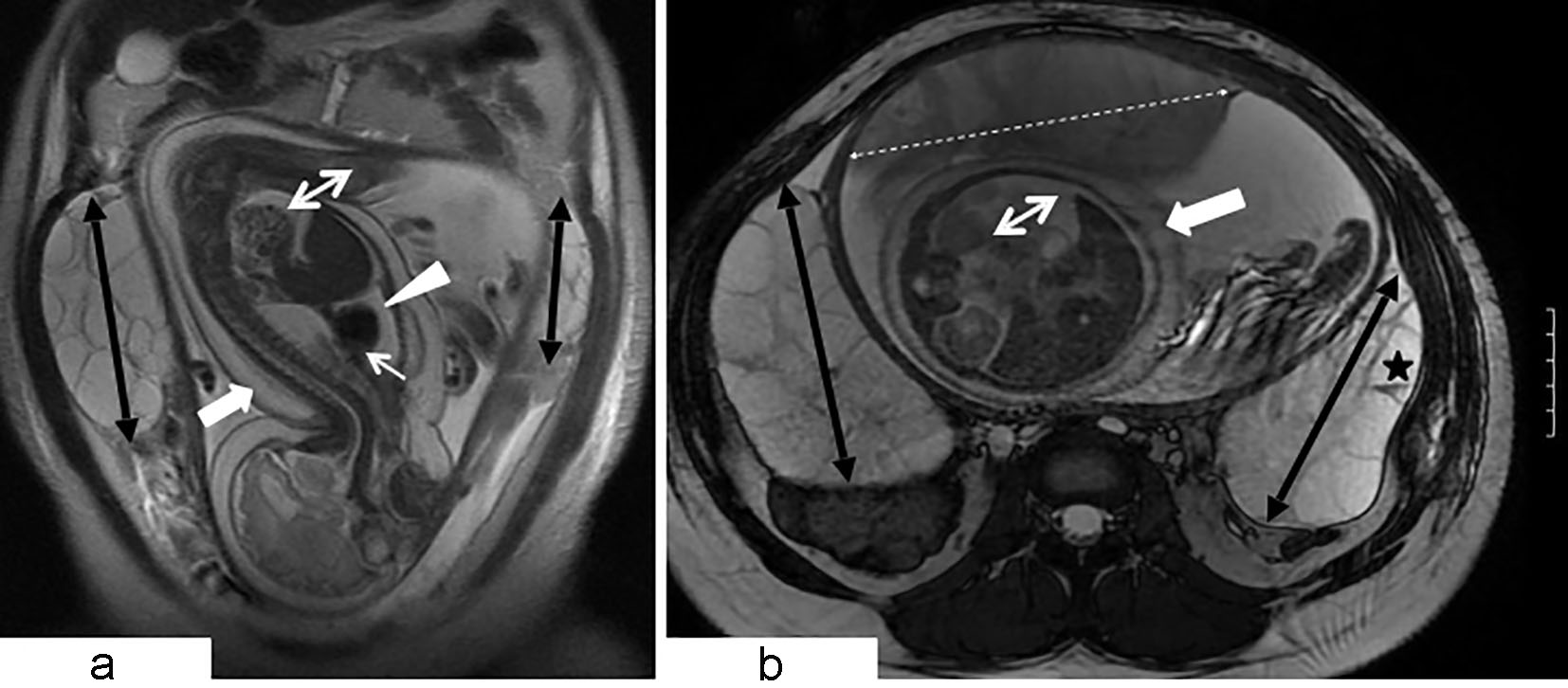
A repeat obstetric ultrasound 2 days later demonstrated an interval increase in ovarian size with the right side measuring 18.5 × 12.6 × 10.2 cm and the left side measuring 12.7 × 11.4 × 8.6 cm. An MRI demonstrated multiple thin walled ovarian cysts without hemorrhagic or fat contents measuring 12.1 × 6.2 × 13.4 cm on the right and 11.1 × 4.8 × 9.5 cm on the left (Fig. 2). An abnormal thickened edematous placenta was seen. There was no pelvic lymphadenopathy. A chest X-ray showed a small pleural effusion. The patient demonstrated no clinical signs of hyperandrogenism such as hirsuitism, deepening of the voice, or clitoromegaly. Electrolytes and albumin were normal. Tumor markers (CA125, CEA, and CA 19-9) were negative. β-hCG levels were elevated to 257,897.9 prior to delivery, and dropped to 5,717.9 on postoperative day 2.
Figure 2. Coronal (a) and axial (b) views of MRI of the abdomen and pelvis (balanced steady state free precession sequence). Large gravid uterus. Cephalic position of hydropic fetus demonstrating diffuse marked skin thickening (large white arrow), large pleural effusion (white arrowhead), moderate pericardial effusion (small white arrow), and ascites (white double arrow). Bilateral flank multiseptated ovarian masses (black double arrows) composed of thin walled cysts. A few cysts reveal small fluid debris level (black star). Thickened enlarged placenta exhibits intermediate T2 signal intensity (white dashed double headed arrow). MRI findings are consistent with bilateral large ovarian theca lutein cysts (hyperreactio luteinalis) and fetal hydrops.
Concomitantly, the hydropic fetus developed a new finding of intermittently reversed A wave in the ductus venosus. Betamethasone was repeated in preparation for delivery.
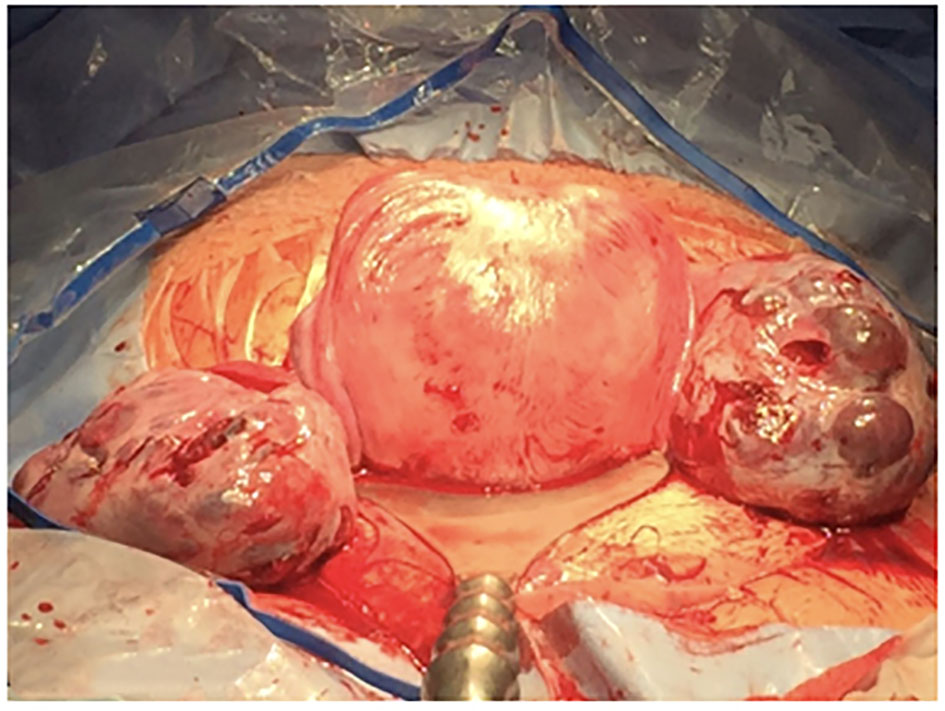
She underwent a primary low transverse Cesarean section at 31 6/7 weeks gestation for abnormal fetal Dopplers, ascites drainage, and bilateral ovarian biopsies. Intraoperative findings demonstrated enlarged multicystic ovaries with the right ovary measuring approximately 15 × 12 cm and the left ovary measuring approximately 12 × 10 cm (Fig. 3). The baby expired a few hours after delivery. Placental pathology showed a normal weight of 482 g and no hydropic change. The left and right ovarian tissue biopsies showed bilateral corpus luteal cysts.
Figure 3. Intraoperative view of the post gravid uterus following cesarean section delivery. Bilateral enlarged ovaries are noted with multiple thin walled theca lutein cysts.
Postoperative input and output along with daily weights were monitored. She developed oliguria, lower extremity edema secondary to third spacing, and early consolidation on chest X-ray from fluid mobilization. She had hypoalbuminemia with a nadir of 1.8 g/dL; other electrolytes were normal. Ultrasound on postoperative day 1 showed the right ovary measuring 10.1 × 9.3 × 8.2 cm and the left ovary measuring 9.5 × 6.7 × 9.5 cm transabdominally, which was slightly smaller than the preoperative MRI measurement.
The patient’s abdominal pain and dyspnea gradually improved postoperatively. Her oliguria and electrolyte imbalance resolved, and she was discharged home in stable condition on postoperative day 4 with plans for repeating an MRI 6 weeks postpartum.
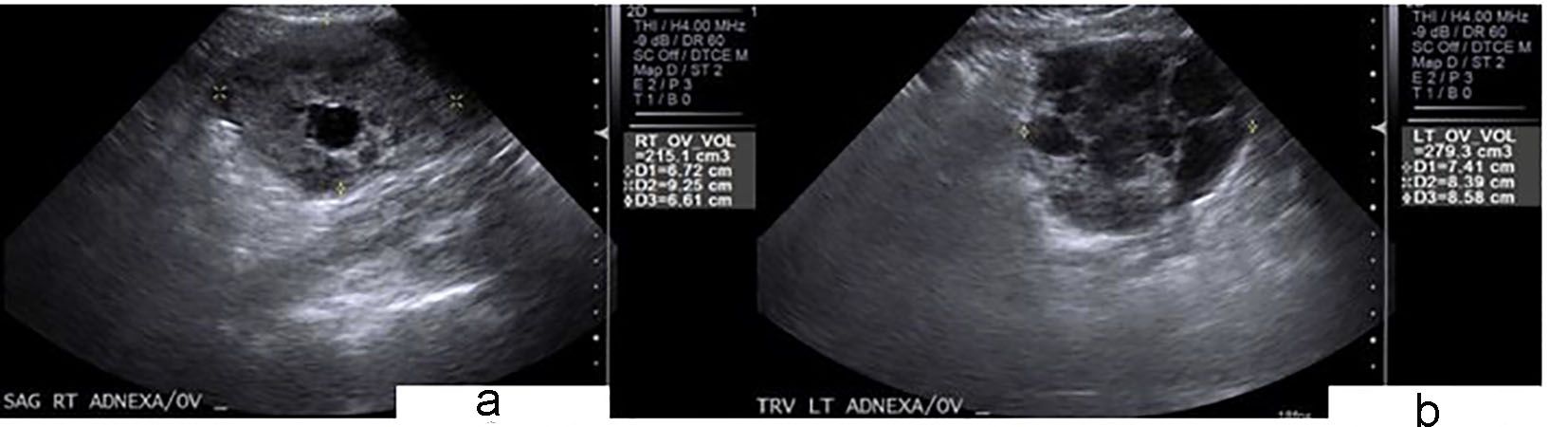
She was readmitted postoperative day 9 with endometritis, and transabdominal ultrasound showed an interval decrease in ovarian size with the right ovary measuring 6.7 × 9.2 × 6.6 cm and the left ovary measuring 7.4 × 8.3 × 8.5 cm (Fig. 4).
Figure 4. Transabdominal ultrasound examination performed 9 days after cesarean section. Interval decreased size of still enlarged right (a) and left (b) ovaries with decreased number of cysts. Right ovary measures 6.7 × 9.2 × 6.6 cm of 215.1 cm3 volume. Left ovary measures 7.4 × 8.3 × 8.5 cm of 279.3 cm3 volume.
Burger described the first case of HL unassociated with trophoblastic disease in 1938; since then there have been 96 reported cases of HL from 1955 to 2013 [3, 4]. The majority of cases (54%) are diagnosed in the third trimester, whereas 16% are diagnosed in the first trimester [4, 5]. HL is asymptomatic in 28% of cases [5]. The most common symptom is lower abdominal pain in 52% of cases due to rapid ovarian growth or hemorrhage into the cysts [4]. Virilization is associated with 25% of cases secondary to elevated androgen levels [5]. Other symptoms and signs include nausea and emesis, pleural effusions, and ascites [4]. Thyroid function is increased in about 33% of cases with suppression of TSH and elevation of free T4 levels [4]. HL can also be associated with preeclampsia. It has been hypothesized that high β-hCG levels can be a marker of placental dysfunction, which can subsequently lead to preeclampsia. Preeclampsia occurs in 24% of HL cases and fetal growth restriction occurs in 12% of cases [4]. Our patient was symptomatic with abdominal pain, and had ascites and a pleural effusion. She demonstrated no clinical signs of hyperandrogenism. Laboratory values showed a low TSH, elevated free and total T3, and a normal free T4 level. Our patient did not develop preeclampsia.
The differential diagnosis of bilateral ovarian enlargement in pregnancy includes OHSS and malignancy. Although OHSS is classically seen secondary to ovulation induction, there have been rare cases associated with spontaneous pregnancies [6, 7]. OHSS typically presents in the first trimester, is associated with rapid ovarian expansion and massive ascites, and is likely due to an exaggerated follicular response from elevated β-hCG levels [7]. Virilization is rarely seen [7]. HL tends to present in the third trimester, follows a more indolent course, has less severe fluid shifts, and often no precipitating factor [5]. HL is associated with virilization in 25% of cases [3, 5]. It may be challenging to differentiate severe HL in the first trimester from spontaneous OHSS as 16% of HL cases are diagnosed in the first trimester [5]. The treatment for both HL and OHSS is aimed at pain control and fluid and electrolyte management [5]. Increased familiarity with the management of HL and OHSS will decrease unnecessary surgery.
HL is characterized by bilateral enlarged ovarian masses that consist of several thin-walled theca lutein cysts with a large solid component on ultrasound. While the large number of locules can be confused with mucinous intestinal borderline tumors, the latter tend to have smaller thin-walled and less rounded locules with less solid tissue [3].
Our case is unique in that it was complicated by mirror syndrome, or Ballantyne syndrome. Mirror syndrome is a severe form of fetal hydrops that is associated with maternal third spacing and edema. It may manifest as ascites or pleural effusions, and is associated with placental edema [8]. Our patient developed ascites and a pleural effusion with severe fetal hydrops leading to our diagnosis. Although rare, mirror syndrome is more likely to occur in early and severe fetal hydrops, and has been reported in 29% of cases [8]. Symptoms and signs included headaches, emesis, mild hypertension, pulmonary edema, and oliguria [8]. Symptoms typically resolve 2 days after delivery, which was consistent with our case [8].
In conclusion, this case highlights some of the key differential diagnoses to be considered in a pregnant patient presenting with large ovarian masses. It also emphasizes the importance of early recognition of HL in guiding conservative management without the need for unnecessary surgical intervention, particularly in young reproductive age females.
Disclosures
I disclose that I have no financial support for the study and have received no funding. An abstract of the case only will be displayed in poster format at the 2017 ACOG Annual Clinical and Scientific Meeting.
Speroff. Clinical Gynecologic Endocrinology and Infertility. Normal and Abnormal Sexual Development. Chapter 9. p. 363-364.
Hoffman, Barbara L, et al. Pelvic Mass. Williams Gynecology, 3 ed. New York, NY: McGraw-Hill, 2016. p. 266.
Van Holsbeke C, Amant F, Veldman J, De Boodt A, Moerman P, Timmerman D. Hyperreactio luteinalis in a spontaneously conceived singleton pregnancy. Ultrasound Obstet Gynecol. 2009;33(3):371-373. doipubmed
Cavoretto P, Giorgione V, Sigismondi C, Mangili G, Serafini A, Dallagiovanna C, Candiani M. Hyperreactio luteinalis: timely diagnosis minimizes the risk of oophorectomy and alerts clinicians to the associated risk of placental insufficiency. Eur J Obstet Gynecol Reprod Biol. 2014;176:10-16. doipubmed
Foulk RA, Martin MC, Jerkins GL, Laros RK. Hyperreactio luteinalis differentiated from severe ovarian hyperstimulation syndrome in a spontaneously conceived pregnancy. Am J Obstet Gynecol. 1997;176(6):1300-1302; discussion 1302-1304. doi
Speroff. Clinical Gynecologic Endocrinology and Infertility. Induction of Ovulation. Chapter 31. p. 1322-1324.
Abe T, Ono S, Igarashi M, Akira S, Watanabe A, Takeshita T. Conservative management of hyperreactio luteinalis: a case report. J Nippon Med Sch. 2011;78(4):241-245. doipubmed
Hirata G, Aoki S, Sakamaki K, Takahashi T, Hirahara F, Ishikawa H. Clinical characteristics of mirror syndrome: a comparison of 10 cases of mirror syndrome with non-mirror syndrome fetal hydrops cases. J Matern Fetal Neonatal Med. 2016;29(16):2630-2634. pubmed
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Clinical Gynecology and Obstetrics is published by Elmer Press Inc.