

| Journal of Clinical Gynecology and Obstetrics, ISSN 1927-1271 print, 1927-128X online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Clin Gynecol Obstet and Elmer Press Inc |
| Journal website http://www.jcgo.org |
Case Report
Volume 1, Number 4-5, October 2012, pages 82-84
Signet Ring Cell of the Non-Neoplastic Endometrium: A Case Report and Literature Review
Sharon Lima, Seung-Yong Seoa, Sung-Chul Lima, b, c
aDepartment of Pathology, School of Medicine, Chosun University, Gwangju, Korea
bResearch Center for Resistant Cells, School of Medicine, Chosun University, Gwangju, Korea
cCorresponding author: Sung-Chul Lim, Department of Pathology, Chosun University Hospital, 588 Seosuk-dong, Dong-gu, Gwangju 501-140, Korea
Manuscript accepted for publication June 14, 2012
Short title: Signet Ring Cell of the Non-Neoplastic Endometrium
doi: https://doi.org/10.4021/jcgo42e
| Abstract | ▴Top |
The observation of signet ring cells in endometrial biopsy results raises the possibility of the existence of a malignant primary or metastatic adenocarcinoma. We describe the case of a middle aged woman whose endometrial biopsy and curettage specimens contained signet ring cells indicating stromal decidual changes. Positive cytokeratin and CD10 immunohistochemistry staining results were revealed in the signet ring cells, features favoring a diagnosis of endometrial stromal cells showing decidual changes rather than a primary or metastatic endometrial neoplasm. Upon immunohistochemistry evaluation, they presented as vacuolated, decidualized endometrial stromal cells. Awareness of this morphologic change in the endometrial stroma can prevent overdiagnosis and overtreatment as primary or metastatic signet ring cell adenocarcinoma. Recognized by this morphologic feature, signet ring cells, or their close mimics, should not always be considered as a high grade or poorly differentiated adenocarcinoma.
Keywords: Signet ring cell; Endometrium; Decidual reaction; Stroma
| Introduction | ▴Top |
A signet ring cell is a round cell having an unexpectedly large central cytoplasmic vacuole which pushes the cell nucleus to the periphery. The vacuoles in these cells can be demonstrated by immunohistochemistry assessment for mucin, the accumulation of glycogen, glycoproteins, and so on. These signet ring cells have been occasionally described as an unusual finding in endometrial histological samples. In 1988, Clement and Scully [1] first described an unusual postmenopausal decidual reaction of the endometrium. Since then, other studies have reported on the topic of signet ring cells of the endometrium, including those found in both neoplastic and non-neoplastic conditions. Using a light microscopic and immunohistochemical features, Iezzoni et al [2] evaluated 5 endometrial biopsy specimens containing signet ring cells that strongly mimicked metastatic or primary adenocarcinoma. Four of the 5 cases seemed to represent altered decidual cells. Two of the cases were postmenopausal patients being treated with progesterone at the time of the biopsy, and in one case the cells had features associated with histiocytes with phagocytic vacuoles. For comparison, the microscopic features of 2 signet ring cell adenocarcinoma cases, metastatic to the endometrium from the breast, were presented. Although once considered synonymous with adenocarcinoma, signet ring cells are now known to occur in a variety of nonadenocarcinomatous neoplasms and in non-neoplastic processes. Because of the low frequency of association with primary tumors, the observation of signet ring cell adenocarcinoma of the endometrium is often indicative of metastatic adenocarcinoma of either gastrointestinal or breast in origin. Thus, the finding of signet ring cells possibly represents decidual, histiocytic or neoplastic conditions. Because of these various possibilities the morphologic evaluation of these cells including immunohistochemical and special mucin staining, and in rare occasions, electron microscopy, is mandatory. The purpose of this case report was to emphasize things that must be considered in the evaluation of endometrial signet ring cells in order to decrease the risk of misdiagnosis and overtreatment.
| Case Report | ▴Top |
We report the case of a 45-year-old woman who presented with painless vaginal spotting over the course of several weeks leading to her visit. A physical examination and computerized tomographic images revealed non-specific findings of the gynecologic solid organs and other portions. She had no past history of tumor or exogenous hormonal therapy. She underwent dilatation and curettage of the endometrium. Grossly, the amount of the curetted tissue and its morphologic features were not specific. Microscopically, the endometrial glands revealed a secretory pattern. The stroma contained loose aggregates of signet ring cells in a state of pre-decidual change, but there was no evidence of cytologic atypia, increased mitotic activity, high nuclear to cytoplasmic ratio or pleomorphism (Fig. 1). Immunohistochemical analysis demonstrated that the signet ring cells were focal reactive for CD10, but not for cytokeratin and CD68 (Fig. 2). Based on the immunohistochemical findings, the signet ring cells found in the endometrium were suspected to be the result of a stromal reaction, suggesting a rare pattern of decidual change.
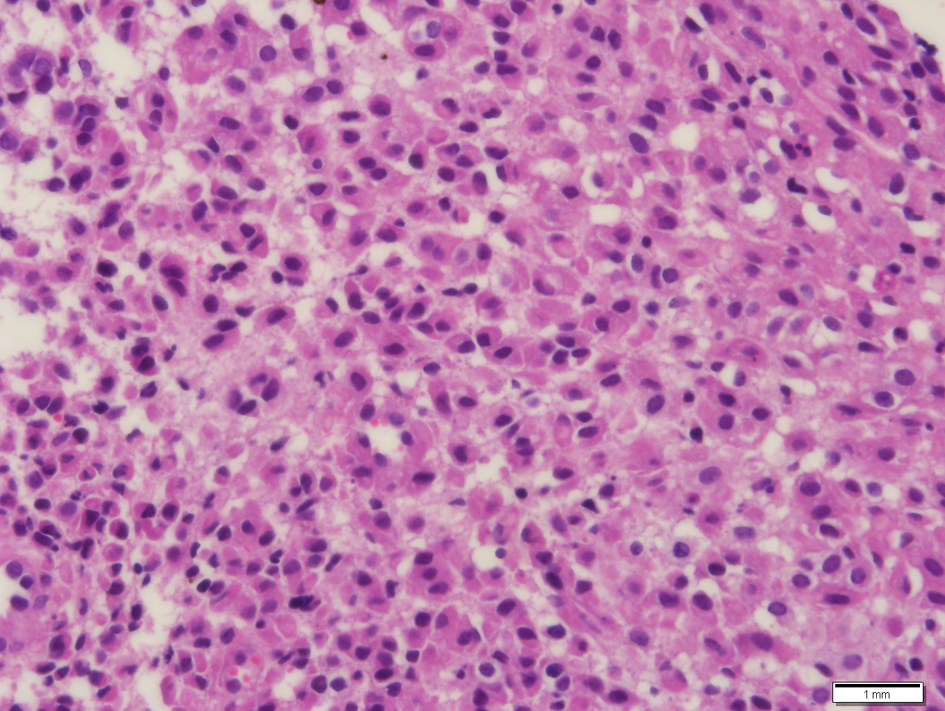 Click for large image | Figure 1. Histopathologic findings of the curetted endometrial biopsy demonstrate diffuse sheet-like signet ring cells in the endometrial stroma. Neither cytologic atypia, nor pleomorphism is identified. Hematoxylin and eosin stain. |
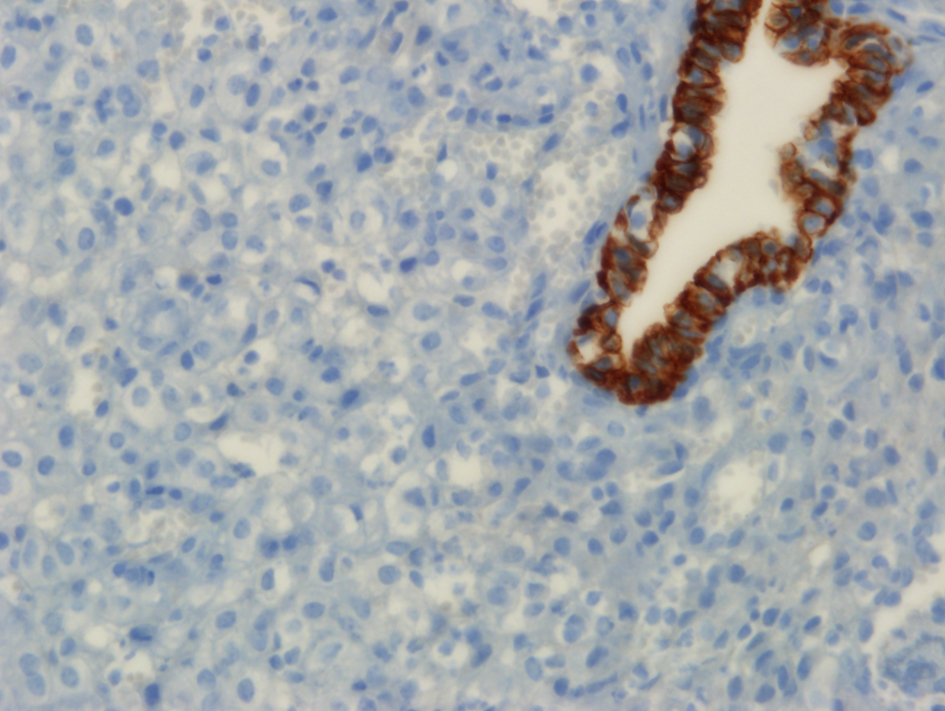 Click for large image | Figure 2. Immunohistochemical staining for cytokeratin shows complete negative reaction in the signet ring cells in the endometrial stroma. By contrast the endometrial gland shows strong positive reaction for cytokeratin. |
| Discussion | ▴Top |
Signet ring cells in an endometrial biopsy are an unusual finding. Signet ring cells, and their close mimics, have prominent or crescent nuclei and variable amounts of cytoplasmic vacuolization or inclusion, ranging from nonvacuolated cells to typical signet ring cells. Signet ring cells of the endometrium are usually representative of the existence of metastatic adenocarcinoma of either breast or gastric in origin. In contrast, true primary signet ring cell carcinomas of the endometrium are extremely rare, but they have been reported [3]. Aside from the neoplastic condition, signet ring cells of the endometrium are associated with a broad spectrum of benign conditions. They are associated with post- or pre-menopausal decidual reactions including hormonal effects, particularly due to progesterone, muciphagic histiocytic differentiation [4] or myxoid changes of cesarean scar endometriosis with massive decidualization [5].
In 1997, the first example of a primary signet ring cell carcinoma of the endometrium was described [3]. This condition can be regarded as a variant of an endometrioid carcinoma because it shows a transition in one area to a conventional endometrioid carcinomatous pattern. However, if a signet ring cell neoplasm is observed in an endometrial biopsy, it is most likely to produce a metastatic gastric carcinoma-signet ring cell type (Krukenberg) tumor. However, the remote possibility of the existence of a primary endometrial neoplasm has to be borne in mind.
Clement and Scully [1] described an unusual postmenopausal decidual reaction of the endometrium including findings with a signet ring cell-like appearance. There was no evidence of an exogenous or endogenous source of excess progesterone in any of the 4 patients. It is possible that, in the four cases, the threshold of the endometrial stromal cells was unusually low, resulting in an increased sensitivity to normal postmenopausal progesterone levels.
Iezzoni et al [2] reported the observation of non-neoplastic signet ring cells in the endometrial biopsies of 5 patients. Three of the 5 patients were in a postmenopausal state, and 2 of the 3 post menopausal patients were receiving hormonal therapy with progesterone. All of these biopsy specimens contained decidual type signet ring cells. In 4 of the cases, the cells were associated with obviously decidualized stromal cells, and there was a morphologic spectrum spanning from nonvacuolated to signet ring cells. All 4 cases were negative for mucin marker, and immunohistochemical nonreactivity for epithelial marker was found, a result consistent with decidual cells. Only the one remaining case of the 5 lacked a background decidual component. The finding consisted of scattered signet ring cells that reacted to histiocytic markers CD68 and Mac387, and the vacuolar contents of the signet ring cells were weakly PAS positive. These cells may have been representative of muciphagic histiocytes. And no evidence of cytologic atypia, increased mitotic activity, high nuclear to cytoplasmic ratio or pleomorphism was observed in any of the 5 reported cases [6].
Prior to performing immunohistochemical staining, obtaining a complete clinical history is the first step in the proper evaluation of a finding of endometrial signet ring cells. The present patient had no specific history of tumor or hormonal therapy, yet non-neoplastic signet ring cells were encountered in the endometrial biopsy. The signet ring cells were surrounded by nonspecific endometrial glands in the secretory phase of menstrual cycle, as determined by histologic dating. The lack of cytologic atypia and negativity for cytokeratin immunostaining seen in the signet ring cell aggregates in the endometrial stroma in this case was suggestive of a rare pattern of decidual change.
The endometrium should join the growing list of anatomical sites potentially harboring non-neoplastic signet ring cells mimicking the tumoral cells associated with metastatic adenocarcinoma. However, negativity for epithelial marker and positivity for endometrial stromal marker, as noted upon immunostaining, were reported in several studies of signet ring cells obtained from the endometrium. Because of the potential for unusual or confused histological findings, additional diagnostic clues are needed in order to make a differential diagnosis between endometrial adenocarcinoma and a decidual change mimicking signet ring cell. Ruling out metastatic adenocarcinoma can be done based on evaluating the spectrum of possible cytologic appearances including blending without atypia, and most important of all, the lack of immunohistochemical reactivity for epithelial markers [7]. The lack of markers is definitely key in distinguishing between metastatic tumors and non-neoplastic signet ring cells of the endometrium.
In conclusion, our patient experienced an extremely rare form of decidual change of the endometrium: a signet ring cell like appearance. The inability to accurately distinguish metastatic or primary signet ring cell carcinoma from signet ring cells of the endometrium is a critical problem. Signet ring cell carcinoma, metastatic or primary, is associated with poor prognosis and requires a more aggressive treatment strategy as compared to unusual signet ring cell like decidual changes.
Disclosures
No Disclosures.
Conflict of Interest
No Conflict of Interest.
| References | ▴Top |
- Clement PB, Scully RE. Idiopathic postmenopausal decidual reaction of the endometrium. A clinicopathologic analysis of four cases. Int J Gynecol Pathol. 1988;7(2):152-161.
pubmed doi - Iezzoni JC, Mills SE. Nonneoplastic endometrial signet-ring cells. Vacuolated decidual cells and stromal histiocytes mimicking adenocarcinoma. Am J Clin Pathol. 2001;115(2):249-255.
pubmed doi - Mooney EE, Robboy SJ, Hammond CB, Berchuck A, Bentley RC. Signet-ring cell carcinoma of the endometrium: a primary tumor masquerading as a metastasis. Int J Gynecol Pathol. 1997;16(2):169-172.
pubmed doi - Jacques SM, Qureshi F, Ramirez NC, Lawrence WD. Unusual endometrial stromal cell changes mimicking metastatic carcinoma. Pathol Res Pract. 1996;192(1):33-36.
pubmed doi - Nogales FF, Martin F, Linares J, Naranjo R, Concha A. Myxoid change in decidualized scar endometriosis mimicking malignancy. J Cutan Pathol. 1993;20(1):87-91.
pubmed doi - Kuhn E, Manoni S, De Anda J. Images in pathology. Signet ring cells in an endometrial biopsy: tumor or not tumor? That is the question. Int J Surg Pathol. 2006;14(3):227.
pubmed doi - Iezzoni JC, Mills SE. Predecidualized signet-ring stromal cells mimicking adenocarcinoma in endometrial biopsy specimens [abstract]. Mod Pathol 1994;7:90A.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Clinical Gynecology and Obstetrics is published by Elmer Press Inc.